
-
Audio not found

It’s been more than 2 1/2 years since one of the worst plane crashes in Minnesota history. That’s a long time for the National Transportation Safety Board to take to investigate an air disaster, even though the “black boxes” were recovered from the wreckage of a corporate jet at the airport in Owatonna (above) in July 2008.
Eight people — the crew and several East Coast business executives — were killed when the jet tried to land, aborted the landing, and then crashed into a cornfield.
“He tried a go around, which is when you land and you know you are not going to make it so you throttle back up and take back off,” eyewitness Brian Mechura told MPR News at the time. “From where I was to the end of the runway was about a mile but it looked like he got up a little bit but when he lifted off the right wing was too heavy. He got it up so the whole airplane from wing tip to wing tip was straight up and down and, the power from the left engine must have forced it around and then it nosed straight in.”
Why? The NTSB is answering that question today at a meeting unveiling the results of the investigation. I’m live blogging the meeting, and you can also watch it here (8:30 CT start).
8:33 a.m. – Deborah Hersman, NTSB chair, is in charge of today’s hearing. “No details is too insignificant to ignore — not the winds, not even the amount of sleep the pilots got. In this case, they all contributed,” she said.
8:35 a.m. – Hersman apologizes to families for the length of time the investigation took, and says that factors were uncovered requiring additional investigation. The abstract of the report will be made available on the NTSB Web site 30 minutes after the conclusion of the meeting.
8:38 a.m. – This is the fourth accident in three years, Hersman says, in which a jet was unable to stop after landing, but it’s the only one in which the pilot attempted to get airborne again.
8:39 a.m. – The presentation begins. John DeLisi, an investigator, begins. Giving a timeline of the investigation. “Early on it became apparent the lack of a flight data recorder was going to hinder our ability to determine performance. The ground proximity warning system provided a limited amount of data.” This conflicts with earlier reports that there were “black boxes” recovered.
8:42 a.m. – DeLisi says there will be 14 safety recommendations as the result of the accident. John Lovell, the investigator in charge, begins his presentation.
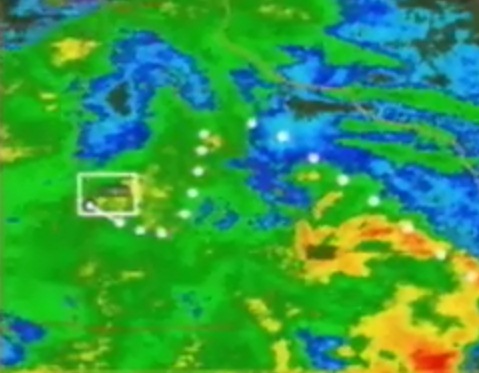
8:44 a.m. – Lovell says the Atlantic City to Owatonna flight was the second leg of a five-leg trip. The captain was flying at the time of the crash. He notes a severe thunderstorm had moved through the region. He says the pilots did not get a weather briefing. The first indication of a weather problem was 20 minutes before landing. A flight controller asked the crew if they saw the ‘extreme precipitation’ 20 miles ahead. He recommended the flight not go through the weather. Seven minutes before landing, he updated the weather for the crew, indicating the winds were from the northwest at 8 knots with thunderstorms in the vicinity.
8:48 a.m. – The crew called the fixed base operator on the ground three times in the last seven minutes. Lovell says the final call — asking about fuel availability — was when the plane was 1,000 feet above the ground. (Bob: That’s not the time to talk about buying fuel)
8:50 a.m. – Here’s the weather at the time, the route of the flight superimposed
8:51 a.m. – The pilot failed to deploy full braking ability for 7 seconds after landing, the plane rolled past the end of the runway, strike a light, took off, and crashed. There was no evidence that hydroplaning occurred.
Bob analysis: That was a pretty blistering indictment of the pilots, even by NTSB standards. It depicted pilots not properly concerned with flying the aircraft safely.
 8:54 a.m. – John O’Callaghan (background – Washington Post) begins his presentation discussing the aircraft. He’s describing the systems on the plane that help it stop. It had no airbrakes, but it had systems in place to create more drag as it rolls to a stop.
8:54 a.m. – John O’Callaghan (background – Washington Post) begins his presentation discussing the aircraft. He’s describing the systems on the plane that help it stop. It had no airbrakes, but it had systems in place to create more drag as it rolls to a stop.
O’Callaghan says newer studies show the plane should have been able to stop in 4,930 feet. But the older “friction model” showed it should have landed in 3,790 feet. The Owatonna runway is only 5,500 feet long. He suggests the newer calculations show the plane should’ve been able to stop if the “lift dump” system were engaged one second after touchdown (the “lift dump” system are the slow-down abilities described earlier). But the pilot didn’t deploy those systems for 7 seconds. O’Callaghan concludes his presentation.
QUESTIONS AND ANSWERS
Q: How slippery was the runway? What role did it play.
A: O’Callaghan: Compared to a dry runway, it was quite slippery. The slipperiness is dependent on the ground speed of the aircraft. It touched down at 130 knots. At that speed, the wet runway renders it very slippery, but not as though it had ice or snow on it.
Q: Was the runway flooded at the time?
A: No.
Q: Was it the old or the new version of the calculation that was in use at the time of the accident?
A: The old one. And that would’ve given improper results.
Q: How could the weather have affected a different approach?
A: The tail wind was a tremendous factor regarding the stopping performance. If the landing had been made into a headwind, the landing distances required would have been significantly reduced. The landing distance would’ve been 4,300 feet down the runway. That’s about the same point where the captain started the attempt to take off again. If he’d landed into the wind, that would’ve been the point at which he stopped.
Q: Some witnesses described a “rooster tail” coming up from behind the airplane…
A: That seemed to be an indication of a lot of water and some flooding. A NASA expert disabused me of that. If you have a rooster tail, it means the tires are in contact with the runway. If you’re hydroplaning, you don’t get a rooster tail. The water you’re seeing is water on the runway but within the macrotexture of the surface. The water is channeled through those.
Q: The calculations seem to require the pilots to be “right on the money” on distance, speed, … if they’re not on the brakes quick, they’re going to absolutely miss that target…
A: That’s correct but that’s where the safety margins are built in (i.e. requiring 1.9 times the landing distance as the calculations suggest one should have).
Q: If the “lift dump” had been deployed within a second of touchdown, the aircraft should’ve stopped at 4,900 feet, is that correct? Even with the tailwind?
A: Yes.
Here’s a chart showing how the the airplane slowed and went off the runway… (click for larger image)
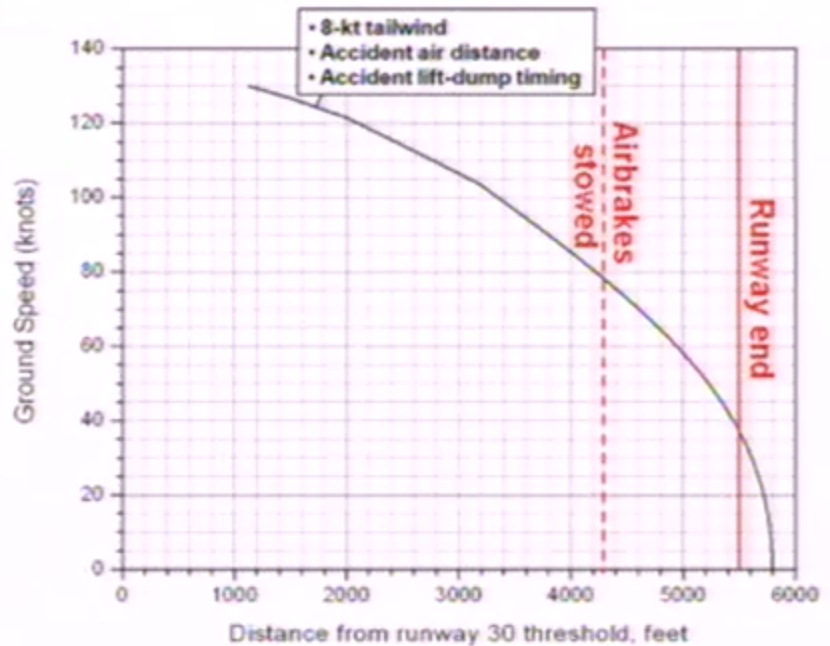
But the plane would’ve stopped if the braking equipment had been deployed sooner. But why wasn’t it? That answer remains to be provided.
Q: We’re talking about a 6 second delay in deploying the “lift dump”?
A: The 7 seconds is measured from the time the nose wheel is on the ground. The one second is from the time the landing gear is on the ground. The difference is about 1.6 seconds. The delay is more like 8 seconds (in this case).
Q: The delay was more like “oops, I thought they’d done that,” more so than not doing it?
A: It’s more than mysterious than that. There was a partial deployment (of the braking mechanism) almost immediately.
Q: If the pilots had done a proper landing distance calculation, would that have given them information not to land?
A: It would’ve given them the OK to land. They were using the old calculations and even with an 8 knot tailwind, it would’ve told them they had enough room to land.
Q: Hersman: What’s concerning to me is if they had conducted the calculations, it would not have told them it was not appropriate to land on this runway.
A: That’s correct. With an 8 knot tailwind using the old model on a wet runway with the safety margin, they had 1,100 feet left.
9:42 a.m. – The pilot was in a card game the night before, got knocked out early, and spent time talking about the runway at Owatonna, wet/dry stopping numbers, the airport diagram, and where to park. They both felt good about the stopping distance. “So he was aware of the numbers,” and investigator said. There’s no indication they updated their calculations prior to the landing.
Q: How do we know the pilots didn’t attempt to deploy the “lift dump” and that it didn’t just fail?
A: We went through the plane from nose to tail and examined everything about that system and we didn’t find any indication of a failure in the system.
PILOTS AND PRACTICES
10:01 a.m. – After a break, the presentation continues. NTSB investigator Capt. Roger Cox is talking about the crew actions.
Cox says there was no formal curriculum for “cockpit resource management” (how pilots and co-pilots work together) at the company East Coast Jets (the charter company) used for training.
He says the pilots had excellent records as individuals, but had significant difference in jet experience.
Bob: These points come up time and time again on crashes like this. It’s the same concerns that were voiced after the Wellstone crash in 2002.
10:09 a.m. – Capt. Cox says the pilot tried to “go around” 17 seconds after touching down, the pilot was not prepared for such an event, and there was no training at the company for how to execute a go-around. (Bob notes: Even the new small plane flying students are taught how to execute a go-around)
10:10 a.m. – The pilots did not have enough weather information available to them to make proper decisions. Unlike airlines, there is no dispatching system for pilots to contact to make those decisions.
10:12 a.m. – Dr. Malcolm Brenner is talking about pilot fatigue now. The pilots got up around 5 a.m. The pilot didn’t go to bed until midnight. They had inadequate sleep. He hints the captain had a sleep disorder. The first officer took sleep medication for which he had no prescription, but got it from his fiance. Dr. Brenner says the performance of the pilots was consistent with fatigue.
QUESTIONS AND ANSWERS
Q: Why did staff choose to call this a “go around” and not a botched landing?
A: Cox: The event was unusual, but the actual actions that he took were consistent with a go-around – Power, flaps, and climb out.
NTSB board member Robert Sumwalt: Pilots are taught that a “go around” maneuver is a safety maneuver. I want to be clear: there is a difference. Anytime you’re in the air, you can and should go around if things don’t look right. But once you put wheels on concrete, you’re committed to stopping. So I don’t want anyone to get the impression that going around is wrong.
Q: In effect, was this a two-crew operation or a single operation?
A: In effect, the pilot took many actions to indicate that he was the sole decision maker. (The suggestion is that the crew wasn’t operating together effectively)
Q: When you evaluate fatigue, what kind of factors do you evaluate?
A: Brenner: Sleep history, how long they’ve been awake, which in this case wasn’t very long; we’re looking at time of day, and medical issues such as a sleep disorder. We also try to evaluate the degree of risk. In this case, they had about 5 hours of sleep, and both them required quite a bit more.
Q: In this case, is this a little bit of sleep loss? Is it significant?
A: Brenner: Comparing this to alcohol, a two-hour cumulative sleep loss can be equivalent to about a .04 blood alcohol percent. Four hours would be closer to .08 percent or in that range.
10:32 a.m. – This captain had a reputation for being very patient with first officers. The first officer in this case had less than 300 hours in this type of jet. Brenner says he interviewed another first officer who had flown with the captain on the Owatonna flight and the captain had instructed him — properly and effectively — on how to land on a short runway. If he had done that in this case, the accident would not have happened. “There should have been a thorough approach briefing. They certainly should’ve talked about the weather and waiting a few minutes. Or ‘if we’re going in, here’s what to look for,'” Brenner said. “The captain on this flight didn’t provide that approach briefing. He seems impatient to get down. It was a different quality… not up to his standards. He also isn’t required to give a briefing.”
Q: Why do you think the captain was impatient to land?
A: Brenner: I don’t know. They were 7 minutes ahead of schedule.
Q: Could it be because they wanted to get down before a thunderstorm hit?
A: Cox: The bulk of it had already passed.
Q: The forecast initially issued for the time of arrival was grossly wrong?
A: The forecast the crew obtained was issued around midnight Atlantic City time. There was no forecast for Owatonna (Bob notes: Aviation forecasts from Minneapolis are used). Once the system raced through the area, the advisories were updated as necessary.
Q: People are paid to forecast accurately. How did they miss it?
A: A briefing would’ve caught that the conditions weren’t quite right. The crew never received an updated forecast (even though) the weather service had updated the forecast.
(Lots of discussion about the failure of the crew to use standardized checklists in preparation for landing)
10:55 a.m. – Sumwalt says the accident reminds him of the Wellstone crash. “In that accident, the NTSB found improper training procedures and lack of crew coordination.”
Cox: During the interviews we asked East Coast Jet pilots about procedures and we got different answers from many of them. Sumwalt says that shows a lack of standardization. “Standardization indicates discipline,” he says. “It’s the backbone of professionalism. If you’re not standardized, you’re not a professional flying organization. You’re just an expensive flying club.” (Bob notes: Ouch. )
10:57 a.m. – Dr. Brenner acknowledges that new rules on crew rest wouldn’t have affected this accident. “They had only been on duty for 5 hours and only been flying for three hours,” he says.
11:02 a.m. – Pilots should’ve been aware they were landing with a tailwind (pilots normally land INTO the wind in order to land with a lower ground speed and reduce the length of runway needed) an hour before the crash occurred.
Sumwalt, an NTSB board member, is lecturing on the “sterile cockpit” rule, which was violated here. Under that rule, non-relevant conversations are prohibited. “There was no reason to be calling the FBO to talk about fuel or anything else, especially when you’re on final approach,” he said.
Q: Summarize the role fatigue played in the accident.
A: Brenner: Both pilots were not at the top of their game. If they’d been more aware of fatigue, they could’ve slept better the night before. The captain was playing a card game at the company at 11 o’clock the night before! For me it’s upsetting that the first officer isn’t getting treatment for insomnia. He was self-medicating. We’ve seen that in other accidents as well.
We feel that the FAA should give a course so there are clear guidelines with the medical group and in your treatment, have a controlled safe use of medications.
(Bob notes: Because the FAA medical office is so restrictive of prescription drugs, a lot of pilots intentionally do not seek medical treatment because they’re afraid they’ll lose their flight status)
Q: We’ve heard a lot about the FAA issuing a notice of proposed rulemaking on fatigue. Would that cover pilots of charters as in this case?
A: No.
Q: Why do we think the crew thought they could execute a takeoff.
A: Brenner: It was an impulsive decision made in high pressure. We can hear in the recording the pilot is breathing heavily. We believe it’s fatigue.
Q: Is it only the pilot’s fault or is it the failure of guidance and training they didn’t have?
A: The procedures of training were inaccurate. We’re not pointing a finger at the pilot and saying he’s soley responsible, but he was the final authority as to the safe conduct of the flight and we felt his interaction with his first officer could have been substantially improved.
(The board is considering a recommendation that once pilots commit to stopping a plane, they don’t take off again)
FINDINGS
The staff is proposing 26 findings:
1) The pilots were properly certificated and qualified.
2) The accident investigation was properly maintained.
3) The accident was not survivable.
4) The captain did not create an atmosphere to guarantee the safety of the flight. Inappropriate conversations, non-standard terminology, no checklist.
5) Poor aeronautic decision-making prevented them from considering alternatives to landing on a wet runway.
6) The airplane touched down within the target touchdown zone and appropriate speed. The captain touched the breaks but failed to deploy a “lift dump” system.
7) If the captain had continued the landing, the accident would’ve been prevented.
8) Establishing a committed-to-stop point would eliminate ambiguity in decision making.
9) No evidence of hydroplaning.
10) If the company had standard operating procedures, many of the contributions to the accident might’ve been corrected.
11) The first officer might’ve been used more effectively had they received crew resource management training as is customary on the airlines.
12) The FAA inspector for East Coast Jets was not familiar with outsourced training.
13) Maintaining consistency between checklists used during training and actual flight is essential to avoiding confusion.
14) Clearly stating and responding to flap settings, rather than saying “set” would eliminate confusion about airplane configuration at a critical moment.
15) Captain didn’t receive proper weather information at Owatonna.
16) If captain had obtained a weather briefing, they would’ve had a more complete weather picture and known they might have to land on a wet runway.
17) Guidance to terms about thunderstorms would allow pilots to make better decisions.
18) Both pilots’ performance was likely caused by fatigue.
19) Although the first officer took a sleep aid, because of the short duration, it’s unlikely the med degraded his performance.
20) Allow civil aviation pilots with insomnia to use sleep medications, would improve abilities.
21) Educating/training pilots on fatigue necessary.
22) Formal training on how pilots can treat fatigue would mitigate incidents.
23) Wet runway guidance in manuals can be significantly shorter than actual distances required to stop on wet runways.
24) Testing requirements for pilots in command are inadequate because they don’t mirror actual flights that charter pilots make.
25) The outdated ground proximity database on the plane was not a factor.
26) A light recording system for airplanes would have helped determine the flight crew’s actions – flap settings, how much breaking effort they made on landing, etc.
Official Cause: The captain’s decision to attempt a go-around late in the landing roll with insufficient runway remaining, poor crew coordination, a lack of cockpit discipline, pilot fatigue, and the failure of the FAA to require cockpit resource training to pilots of Part 135 pilots (charter and business pilots).
12:09 p.m. – NTSB is now debating a recommendation to require pilots to get a weather briefing by phone before flight. I’m not going to bother with that because it’s a little inside baseball. One member says that would delay emergency medical helicopter flights and ignores the reality that weather briefings are available on aviation Web sites, and that weather did not cause this accident.